Fluorescein angiography
Fluorescein angiography
Angiographic appearance varies with the stage of the disease.
It may be identical to classic neovascularization (rarely and more frequently in stage I), with early focal hyperfluorescence (corresponding to the angiomatous formation), leakage and staining, in the intermediate and late stages.
Angiographic appearance in stages II and III is often that of minimally classic or occult membranes.
However, it is very difficult to distinguish between intraretinal neovascularization and choroidal neovascularization or vascularized retinal pigment epithelial (RPE) detachment by FA
(Fig. 1 and 3).
Hot spots normally appear in areas with no window effect, being observed before filling of the RPE detachment with fluorescein.
Stereo FA allows viewing of leakage in the deep retina or the subretinal space(8,19).
The initial stages in the filling of deep vascular lesions and afferent arterioles are often only visible in videoangiography, since filling occurs simultaneously.
Angiomatous lesions may continue to fill even after venous drainage has started(17,19).
Indocyanine green angiography (ICG)
In ICG, a hyperfluorescent focus is visible, which may be observed in all 3 stages, fading only in later stages (Fig. 2).
Late staining or intraretinal oedema, which are typical occurrences in RAP, may also be observed. Intraretinal exudates contain fibrin(18), which may be stained with indocyanine but not with fluorescein.
A hypofluorescent area corresponding to serous RPE detachment may also be observed. With confocal high-speed ICG, early frames allow the establishment of a relationship between RAP and retinal circulation, although without denying the existence of chorioretinal anastomosis(7,10).
High-speed videoangiography also allows identification of retino-retinal anastomoses, chorioretinal anastomoses, feeding arterioles and draining venules (Fig. 2).
Stereo ICG with scanning laser ophthalmoscopy (SLO) shows that RAP consists of a neovascular complex with two components: one is the hot spot (which fills one to three seconds after filling of choroidal arteries, with moderate late leakage); the other consisting of one or more retinal vessels (arteries and particularly veins (70% vs. 30%) (plunging into or emerging from the hot spot)(19).
In stage III, vascularized pigment epithelial detachment (PED) may be observed in ICG.
The serous component of PED is hypofluorescent; the vascular component remains hyperfluorescent.
Figure 1 - RAP lesion
Figure 1 - RAP lesion
Figure 1 - RAP lesion. A: Fundus colour photography (A) with intra-retinal haemorrhages, hard exudates and neurosensory detachment.
Fluorescein angiography shows a retinal hiperfluorescent spot apparently at the end of one retinal vessel, an intra-retinal haemorrhage, neurosensory detachment and pigment epithelium detachment.
Early phase of ICG (C) with an intra-retinal hot spot (angiomatous proliferation) over diffuse choroidal hyperfluorescence.
Late phase ICG (D) reveals a subfoveal hiperfluorescent plaque (subretinal neovascularization).
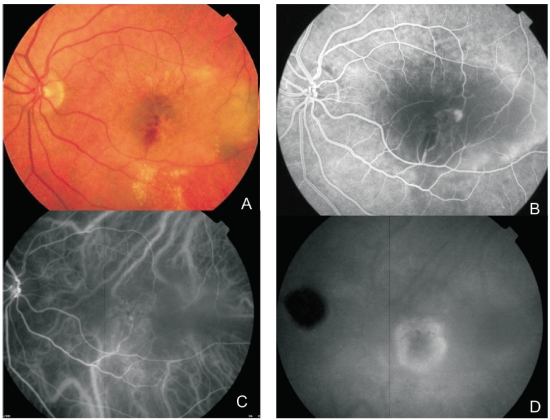
Figure 2 - ICG.
Figure 2 - ICG.
Figure 2 - ICG.
A RAP lesion with retinal-retinal anastomosis, an apparently intraretinal angiomatous mass and a serous PED.
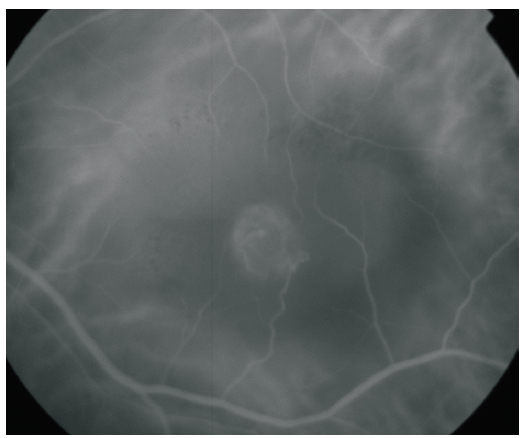
Figure 3 - RAP lesion.
Figure 3 - RAP lesion.
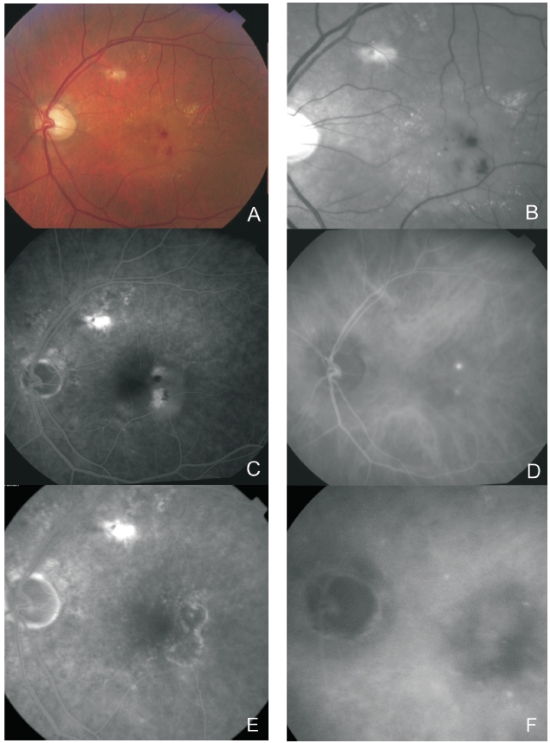
Figure 3 - RAP lesion. Fundus colour photography (A) with intra-retinal haemorrhages, hard exudates and neurosensory detachment.
Red-free (B) with two juxtafoveal and extrafoveal small haemorrhages.
Fluorescein angiography (C) shows two juxtafoveal hyperfluorescent spots, neurosensory detachment and pigment epithelium detachment.
Late ICG reveals two juxtafoveal hyperfluorescent hot spots.
E and F: Fluorescein angiography and ICG after laser photocoagulation with resolution of exudation.