Optical Coherence Tomography Angiography in AMD
Optical Coherence Tomography Angiography in AMD
Authors
João Pedro Marques, MD, MSc
Rufino Silva MD, PhD
Affiliations
Department of Ophthalmology, Centro Hospitalar e Universitário de Coimbra (CHUC), Coimbra, Portugal
Association for Innovation and Biomedical Research on Light and Image (AIBILI), Coimbra, Portugal
Faculty of Medicine, University of Coimbra (FMUC), Coimbra, Portugal
Created in January 2018.
1. BACKGROUND
The advent of optical coherence tomography (OCT) revolutionized retinal imaging by providing a fast, simple, and noninvasive method to assess retinal structure at a microscopic level.(1)
Since its debut more than two decades ago, profound advances in the scanning speed, resolution and image depth led to an explosive growth of OCT in clinical practice, with a significant effect in clinical decision making.(2) Even though technical sophistication improved the OCT diagnostic yield for wet age-related macular degeneration (AMD), there are no agreed-on standards for diagnosing CNV based strictly on cross-sectional OCT(3) and it must ultimately be combined with angiography systems to diagnose CNV accurately. The recent introduction of optical coherence tomography angiography (OCTA), allowed us to redefine our understanding of AMD by conveying three-dimensional, depth-resolved scans of both the superficial and deep retinal capillary plexuses and the choriocapillaris (Video 1). The ability to accurately image CNV noninvasively (Figure 1) and to qualitatively and quantitatively appraise its changes over time (4, 5), turn OCTA into an attractive alternative to conventional dye angiography systems.
Video 1. OCTA allows a three-dimensional depth-resolved view of the retinal and choroidal circulations. This enables us to independently evaluate the vasculature of the inner and outer retina and the choriocapillaris, accurately locating the CNV net, as depicted in this video, recorded with the Optovue Angiovue OCTA system.
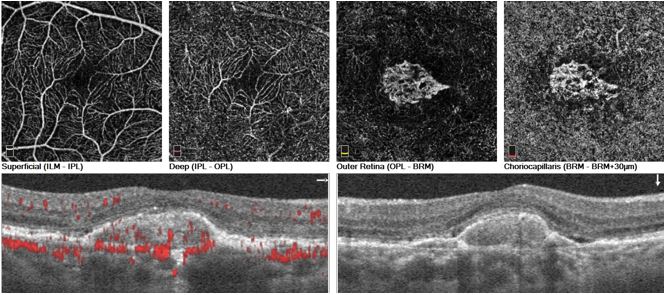
Figure 1. Example of an active CNV lesion imaged with the Optovue Angiovue OCTA system. The superficial and deep retinal plexuses are depicted, along with the outer retina (normally avascular) and the choriocapillaries. Note the presence of a densely packed CNV net composed of loops, peripheral anastomoses and surrounded by a hypointense halo. On SD-OCT, subretinal fluid can be seen.
CNV – choroidal neovasculzarization; SD-OCT – spectral domain optical coherence tomography
2. BRIEF OVERVIEW OF THE TECHNOLOGY
OCTA detects differences in amplitude, intensity or phase variance between a series of sequential B-scans taken at the same location of the retina.(6) The degree of decorrelation in signal is then calculated. This enables visualization of the moving part only, assumed to correspond to the endoluminal flow of erythrocytes within the bloodstream. The above procedure is then repeated for a series of different Y-positions in the retina to achieve the three-dimensional data set, from which proprietary algorithms such as split-spectrum amplitude-decorrelation angiography (SSADA), optical microangiography and OCT angiography ratio analysis are used to reconstruct en face angiograms.(7)
Compared to conventional angiography, OCTA offers several advantages, namely the noninvasive nature and fast acquisition time, thus allowing the exam to be repeated as needed without the added risk of dye injection. In addition, OCTA conveys high-resolution details of the retinal and choroidal microvasculature and a depth-resolved analysis within specific axial locations.(7)
3. OCTA IN EARLY/INTERMEDIATE AMD
The pathogenesis of AMD is known to be associated with inflammation, oxidative damage, ageing, genetic predisposition and environmental factors. However, there is a growing body of evidence implicating choroidal and retinal blood flow in the development of drusen, with hypoxia being associated with the progression of the disease.(8) The advent of OCTA opened doors into the noninvasive evaluation of early/intermediate AMD and has been contributing to a deeper understanding of the disease.
In a recent study, Toto et al(9) used OCTA to evaluate the superficial and deep vessel density of 37 eyes of patients with early (n=14) and intermediate (n=23) AMD. The results were compared to 21 eyes of 21 age- and sex-matched healthy subjects. The authors found a statistically significant difference in both the superficial and deep retinal plexuses between controls and the intermediate AMD group, although not between controls and the early AMD group. These preliminary results corroborate the hypothesis that ischemia plays an important role in the development of AMD. Further studies, preferably longitudinal and with larger populations, are needed to confirm this hypothesis.
Another hallmark of AMD are reticular pseudodrusen (RPD). RPD have been identified as a significant risk factor for late forms of AMD.(10, 11) A recent study used OCTA to evaluate choriocapillaris non-perfusion in early/intermediate AMD eyes with and without RPD.(12) The authors found that eyes with RPD have significantly larger areas of choriocapillaris non-perfusion compared to eyes with drusen and no RPD. Furthermore, the percent choriocapillaris area of non-perfusion (PCAN) strongly correlated with visual acuity, thus providing a potential mechanistic explanation for vision compromise in RPD compared to other forms of drusen in AMD.
4. OCTA IN EXUDATIVE AMD AND ITS NEOVASCULAR PHENOTYPES
Several studies have demonstrated that OCTA can accurately identify type 1 and type 2 neovascularization,(3, 4, 13-16) offering an unrivaled morphological characterization of the choroidal neovascularization (CNV) net that far exceeds FA, ICGA and structural OCT.
Since the OCTA image is not obscured by dye leakage, a clear depiction of the CNV net is provided (Figure 2). Findings from a study by de Carlo et al(3) where 30 eyes with OCTA and same-day FA were evaluated, reported a sensitivity of 50% (4/8) and a specificity of 91% (20/22) for CNV detection with OCTA.
Morphological changes have been reported as the CNV net evolves from active to inactive stages. Characteristic features suggestive of an active CNV net include the presence of a tangle of vessels in a well-defined shape (lacy-wheel, glomerular, sea fan, etc), the presence of anastomoses or loops branching in numerous tiny capillaries, the presence of a peripheral arcade and the presence of a hypointense halo (Figure 3). In contrast, inactive chronic CNVs have larger, more mature vessels, a 'dead tree' appearance with the absence of the anastomoses, loops and peripheral arcades.(13) (Figure 4)
The non-invasive nature of the technique allows comprehensive lesion monitoring after treatment with anti-VEGF compounds. Quantitative measurements of the CNV flow area and flow index reported by Huang et al(17) showed a rapid shutdown of flow over the initial 2 weeks after treatment with anti-VEGF, followed by reappearance of the CNV channel by the fourth week and fluid re-accumulation at 6 weeks. As demonstrated by Lumbroso et al(5) and Marques et al(4), sequential examinations can shadow morphological changes in the neovascular network, closely tracking the timings of vascular network remodeling in patients undergoing treatment (Figure 5). Ultimately, this may allow for the advent of tailored and customized treatment regimens for wet AMD patients, built upon the CNV net morphology at baseline and its response to treatment.(1)
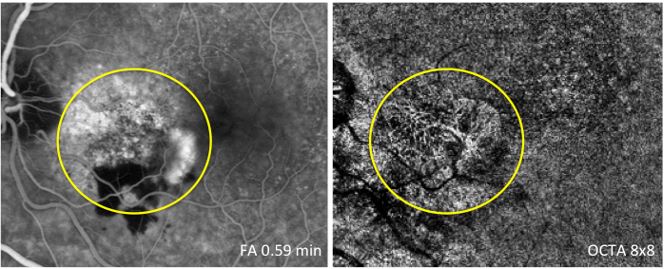
Figure 2. OCTA provides a clear, depth-resolved visualization of the CNV net, not obscured by the staining or pooling effects seen in FA. The image on the right was obtained with the Optovue Angiovue OCTA system.
FA – Fluorescein Angiography; OCTA – Optical Coherence Tomography Angiography; CNV – choroidal neovascularization
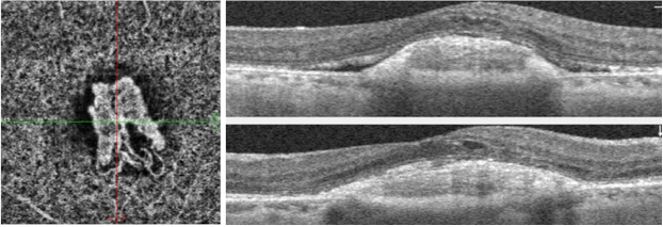
Figure 3. Example of a chronic but still active CNV lesion imaged with the Optovue Angiovue OCTA system. The patient underwent treatment with 8 intravitreal injections of anti-VEGF so far. Note the presence of loops, peripheral arcades and a hypointense halo surrounding the lesion. On SD-OCT, both subretinal and intraretinal fluid can be seen.
CNV – choroidal neovasculzarization; VEGF – vascular endothelial growth factor; SD-OCT – spectral domain optical coherence tomography
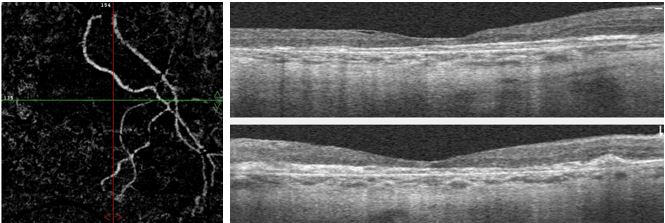
Figure 4. Example of a chronic, inactive CNV lesion imaged with the Optovue Angiovue OCTA system. The larger, more mature vessels are depicted in a 'dead tree' appearance but no peripheral anastomosis or loops are seen. No exudation is visible on SD-OCT and macular atrophy is observed instead.
CNV – choroidal neovasculzarization; SD-OCT – spectral domain optical coherence tomography
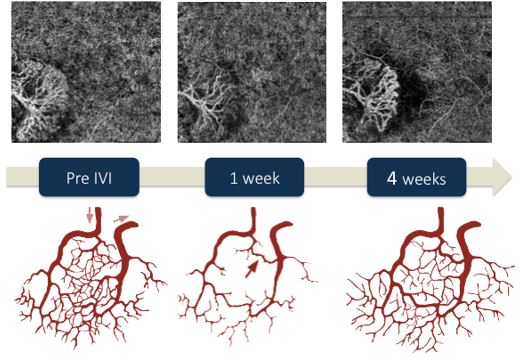
Figure 5. The non-invasive nature of OCTA allows comprehensive lesion monitoring after treatment with anti-VEGF compounds. Sequential examinations can shadow morphological changes in the neovascular network, closely tracking the timings of vascular network remodelling in patients undergoing treatment with anti-VEGF. The image on the left depicts de status of the CNV net before initiating treatment with intravitreal aflibercept. One week after the IVI (middle), marked regression of the peripheral anastomosis and substantial capillary dropout can be seen, along with decreased new vessel density. The feeder trunk and some other central vessels are still visible. Note recanalization of the peripheral anastomosis, resumption of capillary sprouting and increased new vessel density 1 month after the IVI (right). Images acquired with the Optovue Angiovue OCTA system. Adapted with permission from Marques et al (2016).(4)
IVI – intravitreal injection; VEGF – vascular endothelial growth factor
4.1. NONEXUDATIVE CNV
OCTA may also be useful in the screening of eyes at risk for CNV. Unilateral CNV is an established risk factor for the development of neovascularization in the fellow eye. Screening this population for early detection of CNV may have both therapeutic and prognostic implications. A pilot study by Palejwala et al(18) showed that OCTA was able to identify foci of CNV that were not discernible on angiography systems and coined it ‘nonexudative CNV’. OCTA detects CNV by the presence of an abnormal pattern of vascular flow above the Bruch membrane, therefore being able to identify neovascular lesions that do not leak on FA.
A prospective study conducted to determine the natural history of nonexudative CNV found that 23/160 eyes with intermediate AMD had subclinical CNV at presentation (prevalence 14.4%).(19) After the detection of nonexudative CNV, the risk of exudation at 12 months was 15.2 times (95% confidence interval, 4.2-55.4) greater compared with eyes without subclinical CNV. For eyes with nonexudative CNV, recommendations include more frequent follow-up and home monitoring with an amsler grid. So far, intravitreal therapy is not recommended until prospective studies are performed.(19)
4.2. OCTA IN TYPE 3 NEOVASCULARIZATION/RETINAL ANGIOMATOUS PROLIFERATION (RAP)
Qualitative and quantitative analyses of type 3 neovascular complexes can be performed using OCTA.(20, 21) Querques et al(22) evaluated the features of retinal angiomatous proliferation (RAP) with this new imaging modality and found lesions emerging from the deep capillary plexus, forming a clear, tuft-shaped, high-flow network in the outer retinal segment in all eyes, abutting in the sub-RPE space (Figure 6). The authors also reported a small, clew-like lesion present in the choriocapillaris and that, in some cases, this clew-like lesion seemed to be connected to the choroid through a small-caliber vessel. Longitudinal imaging of type 3 neovascularization showed that OCTA could detect changes in the vascular complex even before the presence of exudation on structural OCT. It was also noted that OCTA enabled the distinction between hyper-reflective vascular structures of type 3 neovascularization from hyper-reflective foci devoid of flow, which may correlate to pigment migration.(23) In fact, compared with conventional imaging, OCTA may improve the detection and delineation of vascular changes occurring in type 3 neovascularization (Video 2).
Video 2. Type 3 neovascularization imaged with the Zeiss Angioplex OCTA system. The video shows the presence of the neovascular complex deep in the retina.
A recent study by Martins et al(24), qualitatively and quantitatively evaluated OCTA changes in fellow eyes of type 3 neovascularization. These eyes were shown to have a significantly inferior perfusion density and vessel density in the superficial retinal layer (SRL), deep retinal layer (DRL) and choriocapillaris layer (CL), when compared to both healthy controls and early/intermediate AMD eyes. The authors hypothesized that the compromised vascular perfusion in the CL may be associated with reduced oxygen transport to the RPE and neuro-sensory retina, thus inducing a sub ischemic state that may potentiate the development of RAP.(24). Further longitudinal studies with OCTA may bring additional insights on the pathophysiology of type 3 neovascularization and establish OCTA parameters as biomarkers of this neovascular phenotype of AMD.
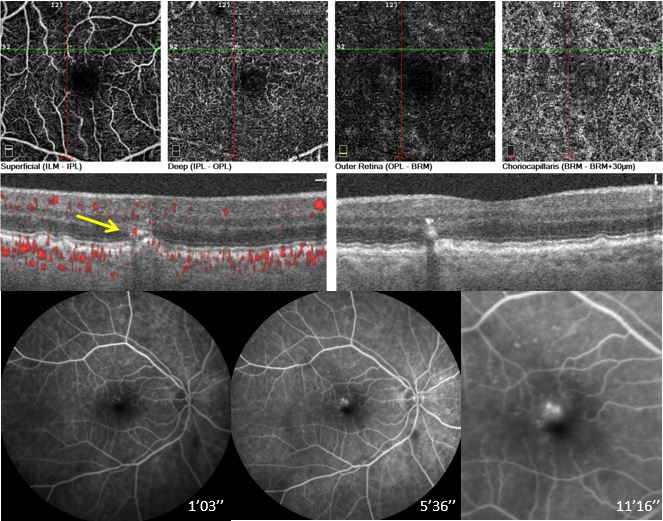
Figure 6. Multimodal imaging of a 73-year old patient with early type 3 NV. OCTA angiogram obtained with the Optovue Angiovue OCTA system (top) shows a large anomalous vessel in the deep retinal plexus (green and red line intersection). The hyper-reflective foci observed on structural SD-OCT (middle) within this particular location have abnormal flow (yellow arrow). However, intraretinal fluid accumulation cannot be seen. Fluorescein angiography (bottom) confirms the presence of an initial type 3 NV lesion with leakage on late phases.
OCTA – optical coherence tomography angioraphy; SD-OCT – spectral domain optical coherence tomography angiography
4.3. OCTA IN POLYPOIDAL CHOROIDAL VASCULOPATHY (PCV)/ANEURISMATIC TYPE 1 NEOVASCULARIZATION
Due to a superior visualization of polyps and branching vascular network (BVN), ICGA has long been the gold standard for the diagnosis of polypoidal choroidal vasculopathy (PCV). Previous studies have shown that OCTA is comparable to ICGA for the detection of the BVN, often showing it with even greater detail than ICGA.(7) On the other hand, the rate of polyp detection by OCTA was much more variable, ranging from 17 to 85%.(25-27) A good example of PCV imaged with OCTA is shown on Video 3.
Video 3. Polypoidal Choroidal Vasculopathy imaged with the Zeiss Angioplex OCTA system. The video shows both the branching vascular network and a polyp. Depending on the position of the slab, the polyp may show either hyperflow or hypoflow. A multimodal evaluation of this patient is shown on Figure 7.
Cross-sectional OCTA of polyps (Figure 7) showed that the lumen is largely devoid of flow.(26, 27) and that the polyp area measured on OCTA was consistently smaller when compared to ICGA.(28) En face OCTA imaging of the polyps was reported to show a more common hypoflow round structure (75%) or less common (25%) hyperflow round structure surrounded by a hypointense halo.(29) It is now widely accepted that the appearance of the polyps on OCTA is highly dependent on the correct positioning of the slab. Some authors hypothesize that the slow or turbulent flow within the polyp may explain its frequently hypoflow appearance.
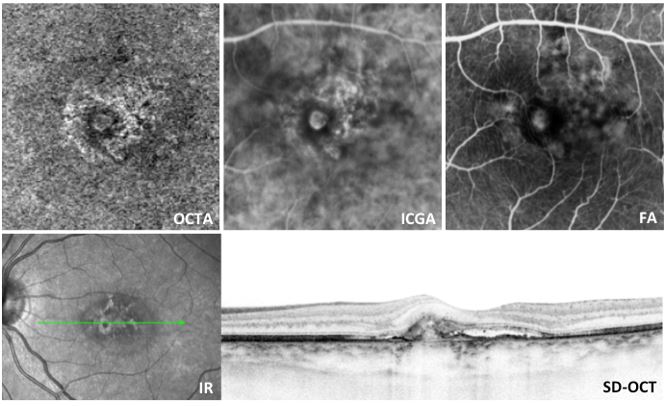
Figure 7.
PCV lesion with a large polyp imaged with OCTA, ICGA, FA and SD-OCT. Note a hypoflow round structure surrounded by a hypointense halo on OCTA. The details and extent of the BVN are better identified on OCTA than ICGA.
OCTA – optical coherence tomography angioraphy; ICGA – indocyanine green angiography; FA – fluorescein angiography; IR – infrared imaging; SD-OCT – spectral domain optical coherence tomography; PCV – polypoidal choroidal vasculopathy; BVN – branching vascular network.
5. OCTA IN GEOGRAPHIC ATROPHY
Geographic atrophy (GA) often follows the disappearance of drusen and is characterized by the well-delineated loss of the RPE, photoreceptors, and choriocapillaris. In fact, late atrophic AMD is an important cause of irreversible vision loss, even in patients with neovascular AMD, because the long-term use of anti-VEGF successfully suppresses neovascularization and results in the progression of these lesions to atrophy.(30)
With the advent of OCTA, it is now possible to visualize the vascular changes that occur in dry AMD (Figures 8 and 9). OCTA shows choriocapillaris flow impairment under the regions of GA.(31-33) In these areas, larger choroidal vessels may be displaced into the area ordinarily occupied by the choriocapillaris and may be seen on the en face OCTA image at the depth level where the choriocapillaris is ordinarily seen.(33) In many cases, the areas of choriocapillaris changes extend beyond the margins of GA in an asymmetric pattern. These changes outside of the margins of GA may be either quite extensive or very limited and subtle.(33) One of the debates regarding choriocapillaris changes in patients with GA is whether they truly represent the absence of flow or merely reduced flow. If the velocity of flow in the vessels is very slow, then OCTA may not be able to detect this slow flow versus the parasitic retinal motion.(33) With the continuous improvement in the software capabilities, this problem will most likely disappear in a near future.
The ability to image the choriocapillaris structure and flow impairments may be useful for detecting and monitoring the progression of dry AMD and for monitoring treatment responses in GA clinical trials.
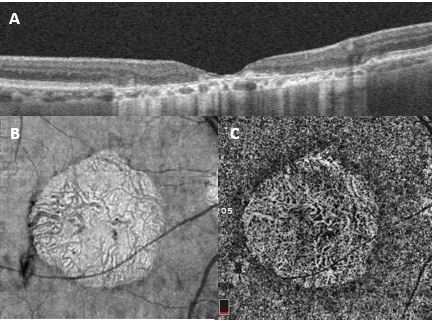
Figure 8. Geographic atrophy (GA) imaged with the Optovue Angiovue OCTA system. The area of GA can be easily observed on structural SD-OCT (A) and on en face OCT (B). Its limits correlate well with the OCTA scan at the level of the choriocapillaris (C). Here, the loss of choriocapillaris allows visualization of the larger choroidal vessels that rest below.
OCTA – optical coherence tomography angioraphy; SD-OCT – spectral domain optical coherence tomography
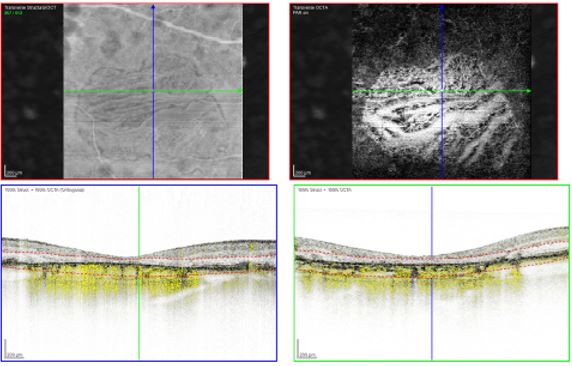
Figure 9. Geographic atrophy (GA) imaged with the Spectralis OCTA system. On the OCTA scan (top right image), the window defect on the choriocapillaris allows visualization of the larger choroidal vessels.
OCTA – optical coherence tomography angioraphy
OCTA ARTIFACTS
Although OCTA merits all the credit for the recent reshaping of our understanding of AMD, attention should be drawn to the appearance of several doubtful findings, mainly related to segmentation errors, ‘ghost images’ due to RPE reflection and the prototype nature of many OCTA devices. The so-called ‘false-friend’ images can induce significant pitfalls in interpreting OCTA scans and lead to unnecessary treatment. (34, 35)
FUTURE PERSPECTIVES
The constant software updates and technical enhancements are making OCTA devices faster, more precise and ultimately more reliable. For instance, the introduction of 3D projection artifact removal and the incorporation of tools to quantitative evaluate vessel density, perfusion/non perfusion, etc increased the usefulness and trustworthiness of OCTA. We believe that this will further reduce the use of conventional angiographic systems, turning OCTA in the gold standard for diagnosis, managing and monitoring of AMD and other retinal diseases. Reading centres around the world are beginning to work with this technology and the inclusion of OCTA images in clinical trials will most likely lead to the advent of OCTA biomarkers of AMD progression and treatment response.
Furthermore, the combination of OCTA and OCT Leakage (OCT-L) seems particularly promising in order to evaluate both vessel parameters and fluid accumulation non-invasively.(36, 37)
CONCLUSION
We embark on a new era of retinal imaging with great expectations in mind, hoping that OCTA can point out new clinical coordinates to improve the everyday management of AMD patients.
References of Optical Coherence Tomography in Age-related Macular Degeneration
References of Optical Coherence Tomography in Age-related Macular Degeneration
REFERENCES
- Marques JP, Silva R. Optical coherence tomography angiography in wet age-related macular degeneration (AMD). Eye Sci. 2016.
- Puliafito CA. OCT angiography: the next era of OCT technology emerges. Ophthalmic surgery, lasers & imaging retina. 2014;45(5):360.
- de Carlo TE, Bonini Filho MA, Chin AT, Adhi M, Ferrara D, Baumal CR, et al. Spectral-domain optical coherence tomography angiography of choroidal neovascularization. Ophthalmology. 2015;122(6):1228-38.
- Marques JP, Costa JF, Marques M, Cachulo ML, Figueira J, Silva R. Sequential Morphological Changes in the CNV Net after Intravitreal Anti-VEGF Evaluated with OCT Angiography. Ophthalmic research. 2016;55(3):145-51.
- Lumbroso B, Rispoli M, Savastano MC. Longitudinal Optical Coherence Tomography-Angiography Study of Type 2 Naive Choroidal Neovascularization Early Response after Treatment. Retina. 2015;35(11):2242-51.
- Gao SS, Jia Y, Zhang M, Su JP, Liu G, Hwang TS, et al. Optical Coherence Tomography Angiography. Investigative ophthalmology & visual science. 2016;57(9):OCT27-36.
- Tan ACS, Tan GS, Denniston AK, Keane PA, Ang M, Milea D, et al. An overview of the clinical applications of optical coherence tomography angiography. Eye. 2017.
- Remsch H, Spraul CW, Lang GK, Lang GE. Changes of retinal capillary blood flow in age-related maculopathy. Graefe's archive for clinical and experimental ophthalmology = Albrecht von Graefes Archiv fur klinische und experimentelle Ophthalmologie. 2000;238(12):960-4.
- Toto L, Borrelli E, Di Antonio L, Carpineto P, Mastropasqua R. Retinal Vascular Plexuses' Changes in Dry Age-Related Macular Degeneration, Evaluated by Means of Optical Coherence Tomography Angiography. Retina. 2016;36(8):1566-72.
- Gil JQ, Marques JP, Hogg R, Rosina C, Cachulo ML, Santos A, et al. Clinical features and long-term progression of reticular pseudodrusen in age-related macular degeneration: findings from a multicenter cohort. Eye. 2017;31(3):364-71.
- Hogg RE, Silva R, Staurenghi G, Murphy G, Santos AR, Rosina C, et al. Clinical characteristics of reticular pseudodrusen in the fellow eye of patients with unilateral neovascular age-related macular degeneration. Ophthalmology. 2014;121(9):1748-55.
- Nesper PL, Soetikno BT, Fawzi AA. Choriocapillaris Nonperfusion is Associated With Poor Visual Acuity in Eyes With Reticular Pseudodrusen. American journal of ophthalmology. 2017;174:42-55.
- Coscas GJ, Lupidi M, Coscas F, Cagini C, Souied EH. OPTICAL COHERENCE TOMOGRAPHY ANGIOGRAPHY VERSUS TRADITIONAL MULTIMODAL IMAGING IN ASSESSING THE ACTIVITY OF EXUDATIVE AGE-RELATED MACULAR DEGENERATION: A New Diagnostic Challenge. Retina. 2015;35(11):2219-28.
- Moult E, Choi W, Waheed NK, Adhi M, Lee B, Lu CD, et al. Ultrahigh-speed swept-source OCT angiography in exudative AMD. Ophthalmic surgery, lasers & imaging retina. 2014;45(6):496-505.
- Jia Y, Bailey ST, Wilson DJ, Tan O, Klein ML, Flaxel CJ, et al. Quantitative optical coherence tomography angiography of choroidal neovascularization in age-related macular degeneration. Ophthalmology. 2014;121(7):1435-44.
- Kuehlewein L, Bansal M, Lenis TL, Iafe NA, Sadda SR, Bonini Filho MA, et al. Optical Coherence Tomography Angiography of Type 1 Neovascularization in Age-Related Macular Degeneration. American journal of ophthalmology. 2015;160(4):739-48 e2.
- Huang D, Jia Y, Rispoli M, Tan O, Lumbroso B. Optical Coherence Tomography Angiography of Time Course of Choroidal Neovascularization in Response to Anti-Angiogenic Treatment. Retina. 2015;35(11):2260-4.
- Palejwala NV, Jia Y, Gao SS, Liu L, Flaxel CJ, Hwang TS, et al. Detection of Nonexudative Choroidal Neovascularization in Age-Related Macular Degeneration with Optical Coherence Tomography Angiography. Retina. 2015.
- de Oliveira Dias JR, Zhang Q, Garcia JMB, Zheng F, Motulsky EH, Roisman L, et al. Natural History of Subclinical Neovascularization in Nonexudative Age-Related Macular Degeneration Using Swept-Source OCT Angiography. Ophthalmology. 2017.
- Kuehlewein L, Dansingani KK, de Carlo TE, Bonini Filho MA, Iafe NA, Lenis TL, et al. Optical Coherence Tomography Angiography of Type 3 Neovascularization Secondary to Age-Related Macular Degeneration. Retina. 2015;35(11):2229-35.
- Tan AC, Dansingani KK, Yannuzzi LA, Sarraf D, Freund KB. Type 3 Neovascularization Imaged with Cross-Sectional and En Face Optical Coherence Tomography Angiography. Retina. 2016.
- Querques G, Miere A, Souied EH. Optical Coherence Tomography Angiography Features of Type 3 Neovascularization in Age-Related Macular Degeneration. Dev Ophthalmol. 2016;56:57-61.
- Tan AC, Dansingani KK, Yannuzzi LA, Sarraf D, Freund KB. Type 3 Neovascularization Imaged with Cross-Sectional and En Face Optical Coherence Tomography Angiography. Retina. 2017;37(2):234-46.
- Martins A, Farinha C, Raimundo M, Lopes M, Santos AR, Melo P, et al. Multimodal Evaluation of the Fellow Eye of Patients with Retinal Angiomatous Proliferation. Ophthalmic research. 2017.
- Inoue M, Balaratnasingam C, Freund KB. Optical Coherence Tomography Angiography of Polypoidal Choroidal Vasculopathy and Polypoidal Choroidal Neovascularization. Retina. 2015.
- Tanaka K, Mori R, Kawamura A, Nakashizuka H, Wakatsuki Y, Yuzawa M. Comparison of OCT angiography and indocyanine green angiographic findings with subtypes of polypoidal choroidal vasculopathy. The British journal of ophthalmology. 2017;101(1):51-5.
- Tomiyasu T, Nozaki M, Yoshida M, Ogura Y. Characteristics of Polypoidal Choroidal Vasculopathy Evaluated by Optical Coherence Tomography Angiography. Investigative ophthalmology & visual science. 2016;57(9):OCT324-30.
- Takayama K, Ito Y, Kaneko H, Kataoka K, Sugita T, Maruko R, et al. Comparison of indocyanine green angiography and optical coherence tomographic angiography in polypoidal choroidal vasculopathy. Eye. 2017;31(1):45-52.
- Srour M, Querques G, Semoun O, El Ameen A, Miere A, Sikorav A, et al. Optical coherence tomography angiography characteristics of polypoidal choroidal vasculopathy. The British journal of ophthalmology. 2016;100(11):1489-93.
- Velez-Montoya R, Oliver SC, Olson JL, Fine SL, Mandava N, Quiroz-Mercado H. Current knowledge and trends in age-related macular degeneration: today's and future treatments. Retina. 2013;33(8):1487-502.
- Moult EM, Waheed NK, Novais EA, Choi W, Lee B, Ploner SB, et al. Swept-Source Optical Coherence Tomography Angiography Reveals Choriocapillaris Alterations in Eyes with Nascent Geographic Atrophy and Drusen-Associated Geographic Atrophy. Retina. 2016;36 Suppl 1:S2-S11.
- Kvanta A, Casselholm de Salles M, Amren U, Bartuma H. Optical Coherence Tomography Angiography of the Foveal Microvasculature in Geographic Atrophy. Retina. 2017;37(5):936-42.
- Waheed NK, Moult EM, Fujimoto JG, Rosenfeld PJ. Optical Coherence Tomography Angiography of Dry Age-Related Macular Degeneration. Dev Ophthalmol. 2016;56:91-100.
- Spaide RF, Fujimoto JG, Waheed NK. Image Artifacts in Optical Coherence Tomography Angiography. Retina. 2015.
- Coscas G, Lupidi M, Cagini C, Coscas F. 'False-friend' images on optical coherence tomography angiography: early choroidal neovascularization or artefact? Acta ophthalmologica. 2016.
- Farinha C, Santos T, Marques IP, Marques JP, Ribeiro L, Figueira J, et al. OCT-Leakage Mapping. Ophthalmology Retina.1(6):486-96.
- Cunha-Vaz J, Santos T, Ribeiro L, Alves D, Marques I, Goldberg M. OCT-Leakage: A New Method to Identify and Locate Abnormal Fluid Accumulation in Diabetic Retinal Edema. Investigative ophthalmology & visual science. 2016;57(15):6776-83.